
At the Tuesday, January 11 meeting of the Public Health and Social Services Committee, we heard from a delegate who – at least based on their social media presence and previous delegations to committee/council – appears (at minimum) to be anti-vax, anti-mask, and anti-lockdown.
The delegate was on the agenda to present at the December meeting of the same committee, but the committee voted to not hear the presentation. I was not present at the meeting, having sent my regrets, and I have not watched the video, so I’m not entirely sure how this came to pass, except that there was an e-mail from the Niagara Health System that drew attention to various points of misinformation (about Niagara Health System) in the delegate’s presentation.
I have indicated publicly that I have serious reservations about providing a platform to people whose information we know to be false and/or presented in a way that is incorrect and for reasons that may be disingenuous and cause harm to our communities. By virtue of providing the platform, we lend them credibility.
Several people have asked me why we would: 1. permit someone to waste our time; and/or 2. why we would engage with them following their presentation.
There are two key points to raise here:
- There is no mechanism or process by which we can measure the validity, reliability, truthfulness, or motives for someone’s presentation. And should we? (I’ll leave that for you to ponder, but it strikes me as a slippery slope.)
- Engaging with them is the only way to ensure that correct information (if that’s our problem with the presentation) is communicated. Let me explain.
In this particular instance, the delegate appears to have been using reliable sources of data. It was their interpretation of the data that was convenient (for their purposes) or interpreted incorrectly.
When the delegate spoke about mortality rates, they only spoke about mortality rates up to the age of 49 years old. (There was a brief mention of the recovery rate for 70+, but it was very brief; not in the presentation being shown to the public; and incorrect.)
And, yes, the mortality rate for those who are younger than 49 years old is decent (but, then, in my view, was also need to have a discussion about what is one’s “magic number,” i.e., how much death is “acceptable”?).
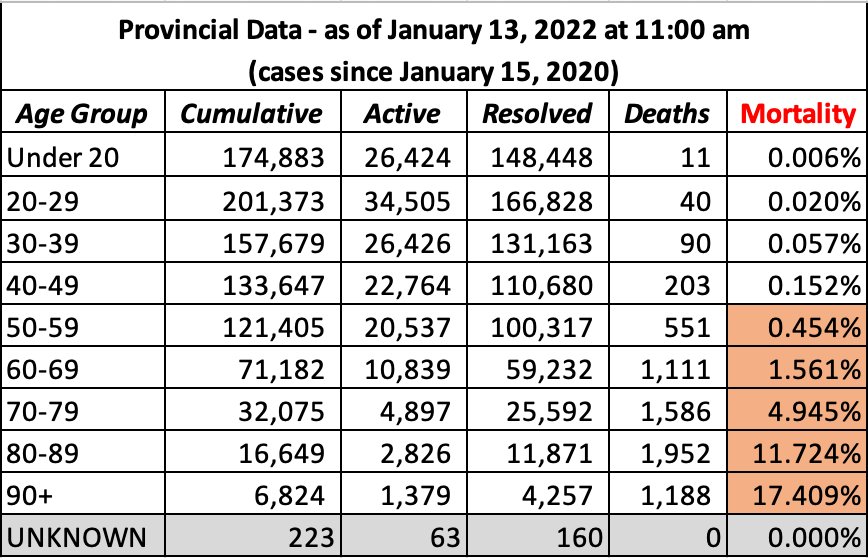
You can see that the mortality rate for those 49 years old and younger who contract COVID-19 is much less than 1%; however, you can also see that it increases significantly as one who contracts COVID-19 increases in age.
Now, there are some in the community who have expressed that they are fine with the deaths of older people and ‘they probably have co-morbidities anyway’ and ‘we don’t know if COVID-19 is what killed them or if it was one of their co-morbidities.’ Yes, these are e-mails that I continue to receive.
I, however, am not fine with someone dying from something that is preventable or at least much more manageable (if the appropriate public health measures are taken), regardless of their age or health status.
The delegate also claimed that vaccines do not work, because – if they did work – we would not be seeing more vaccinated people in hospital than unvaccinated. It is true that there are more vaccinated people in hospital than unvaccinated.
What the delegate did not discuss, though, was the ratio of patients in the vaccinated population versus the ratio of patients in the unvaccinated population.
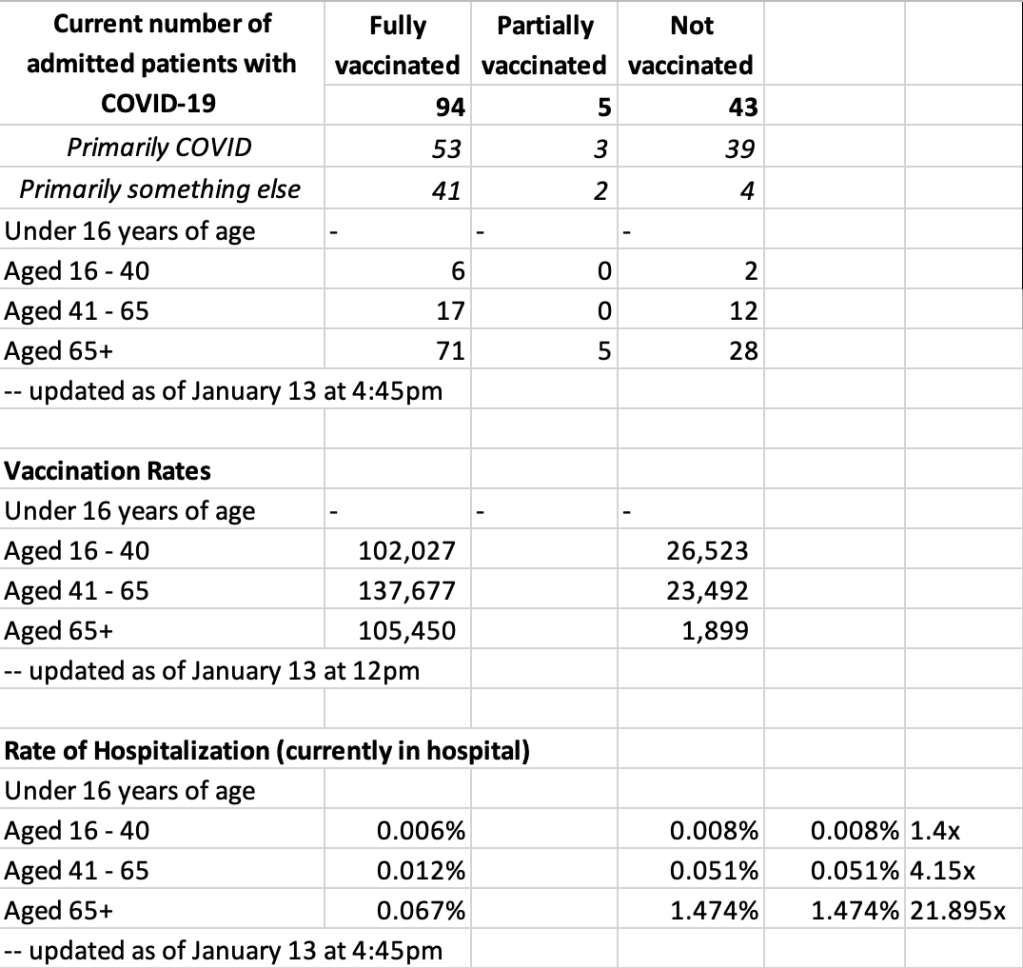
Now, there is – admittedly – a little bit of what I will call ‘slippage’ in the numbers in this spreadsheet above, because The Niagara Health System and Niagara Region Public Health do not use the same age groups. Also, there is no publicly available and clear count of how many people are partially vaccinated, but the percentage is very small.
However, what is shown here is that, for instance, if you are 65+ and you are unvaccinated (as approximately 1,899 people in this population are) and you contract COVID-19, you are – based on today’s numbers – 21.895 TIMES MORE LIKELY to end up in hospital than your 65+ vaccinated (105,450 people in this population) who contracts COVID-19.
If you are in the 41-65 age group and you are unvaccinated (as approximately 23,492 people in this population are) and you contract COVID-19, you are – based on today’s numbers – 4.15 TIMES MORE LIKELY to end up in hospital than your vaccinated counterparts in the same age group who contract COVID-19. Maybe 4.15 times does not seem like a big risk. I know it’s not a risk I’m willing to take.
I engaged with the delegate to ask them if they were aware of these statistics. (I did this in the form of questions, because – and as I explained to the delegate prior to beginning to ask my questions – our Procedural By-Law permits us only to ask questions; not to debate with the delegate.) By engaging and asking the questions I did, I used the same platform from which the delegate’s presentation was given to ensure that correct and complete information was communicated to the public.
If we are going to provide a platform from which people can spread misinformation, then we have a responsibility to ensure that we are countering that misinformation by communicating correct information.
